The superior inferior
 I would say that the most frightening, cluster inducing type of heart attack is the inferior MI, which is also the most deadly, 80% of patients with this condition die. The tricky part about them that instead of responding well to nitrates (the usual treatment for heart attacks), these patients drop their blood pressure precipitously instead. Potentially to the point of death.
I would say that the most frightening, cluster inducing type of heart attack is the inferior MI, which is also the most deadly, 80% of patients with this condition die. The tricky part about them that instead of responding well to nitrates (the usual treatment for heart attacks), these patients drop their blood pressure precipitously instead. Potentially to the point of death.We got called for chest pain and when we arrived we found a guy, laying in bed, so wet with sweat that it looked like he had stepped out of the rain, complaining of severe chest pain. From the start this call had potential. He had been outside mowing the grass, developed this pain and stopped, hoping it would go away. At this point he went upstairs. Why? I couldn't tell you. Then he took three of is prescription nitros. Hence the laying down and the blood pressure of 80 palp.
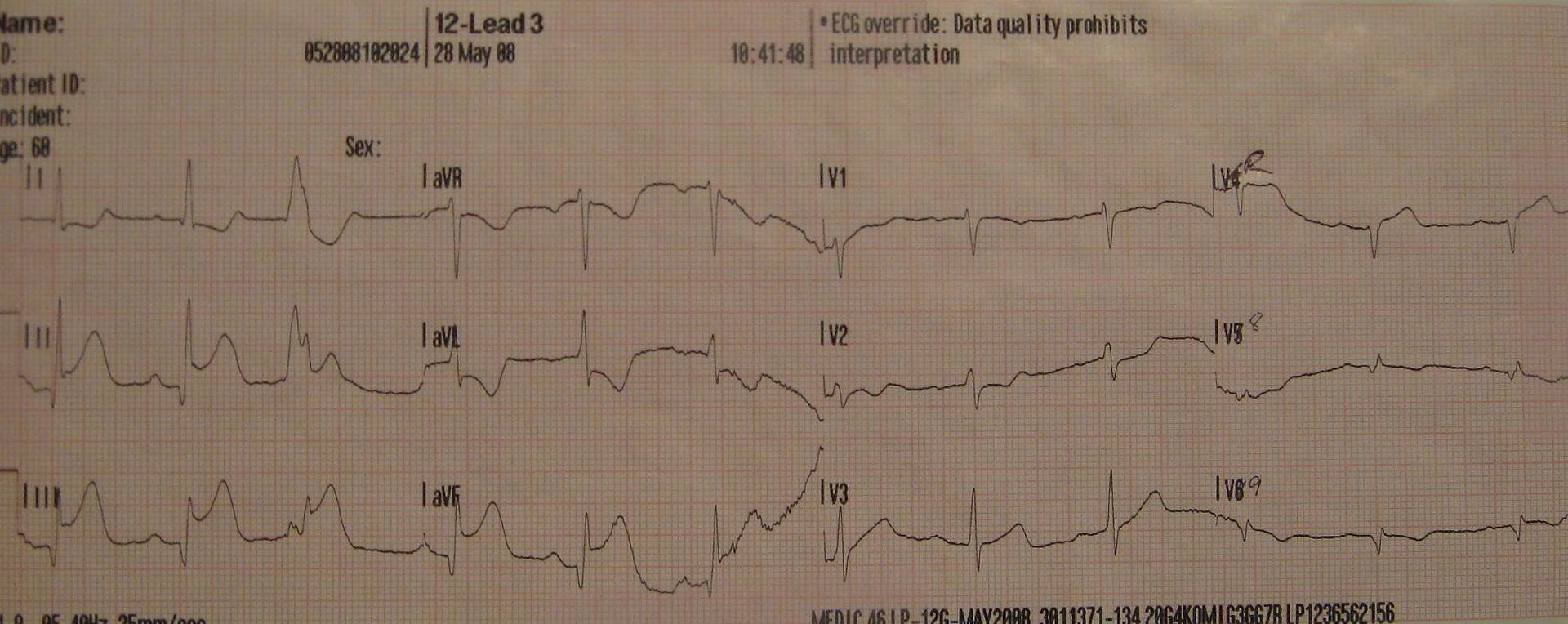
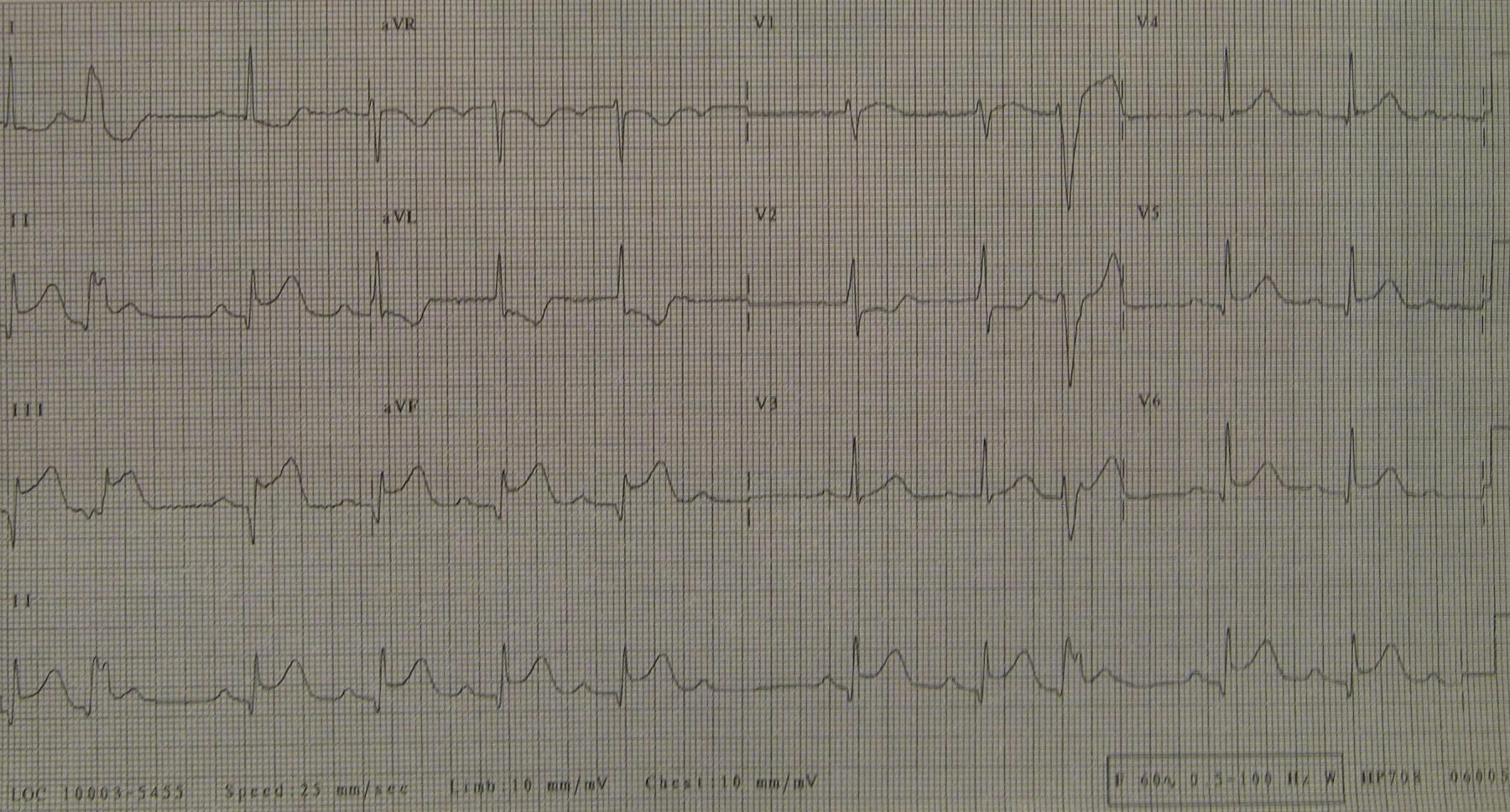
We immediately put him on the monitor which showed what is called a third degree atrio-ventricular heart block. Basically, this patients atria (the top of the heart) and his ventricles (the bottom of the heart) were pumping at different rates, totally independent of eachother. This is very unusual and very bad. We ran a 12 lead and found ST elevation (indicative of a heart attack) in the inferior leads. Oh crap. This is also very unusual and very bad. We started a line right there and began putting fluids in him. Getting down his narrow winding stairs was an experience in itself, and I think nearly killed at least one EMT. When we did successfully get him outside and in the ambo, I had to wipe the sweat off of him and got another 12 lead (pictured below) My partner started another line, gave him aspirin and I got a 15 lead (pictured below) which is a fun thing to do, and gives me even more areas of the heart to look at. That one didn't look too great either. The prehospital treatment for a heart attack like this is fluids, and I mean a lot of them. I called the doc and thankfully he took my word for it and was ready when we arrived at the hospital.
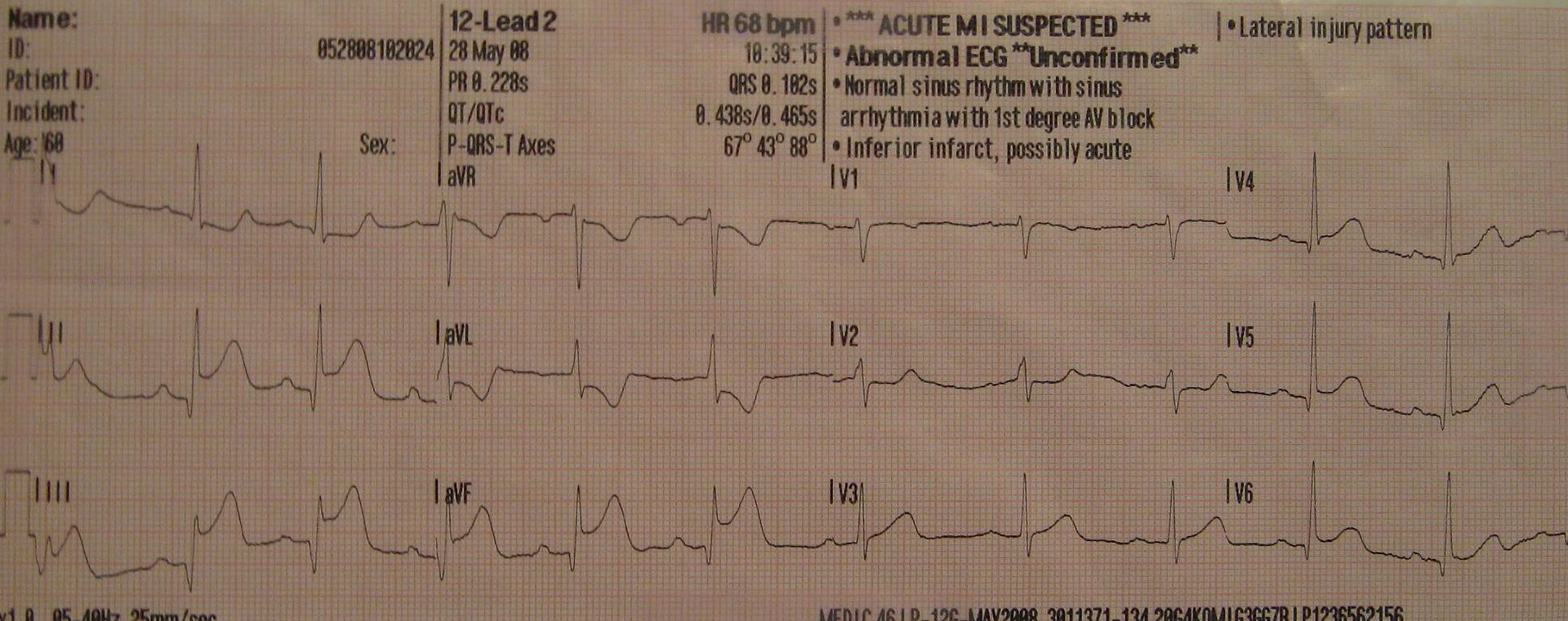
2nd 12 lead
15 lead
About two minutes after we got there, a helicopter was called to take the patient to an interventional cath lab. About three minutes after that the patient coded and went into ventricular fibrillation. Very bad. I was restocking when I head them call it in his room. I ran in in time to see them shock him once and he came back to life. Conscious and alert. "How do you feel?!" "Better." Better?! You just got shocked with 360 Jules, and you feel better?! That was freaking awesome. Thankfully someone was explaining all this to his wife, who, I'm afraid didn't get that we were in quite a hurry on scene. I always stop and talk to the family before we leave. "We may be in a hurry, but you don't need to be. Drive safely to the hospital, okay?" She calmly agreed.
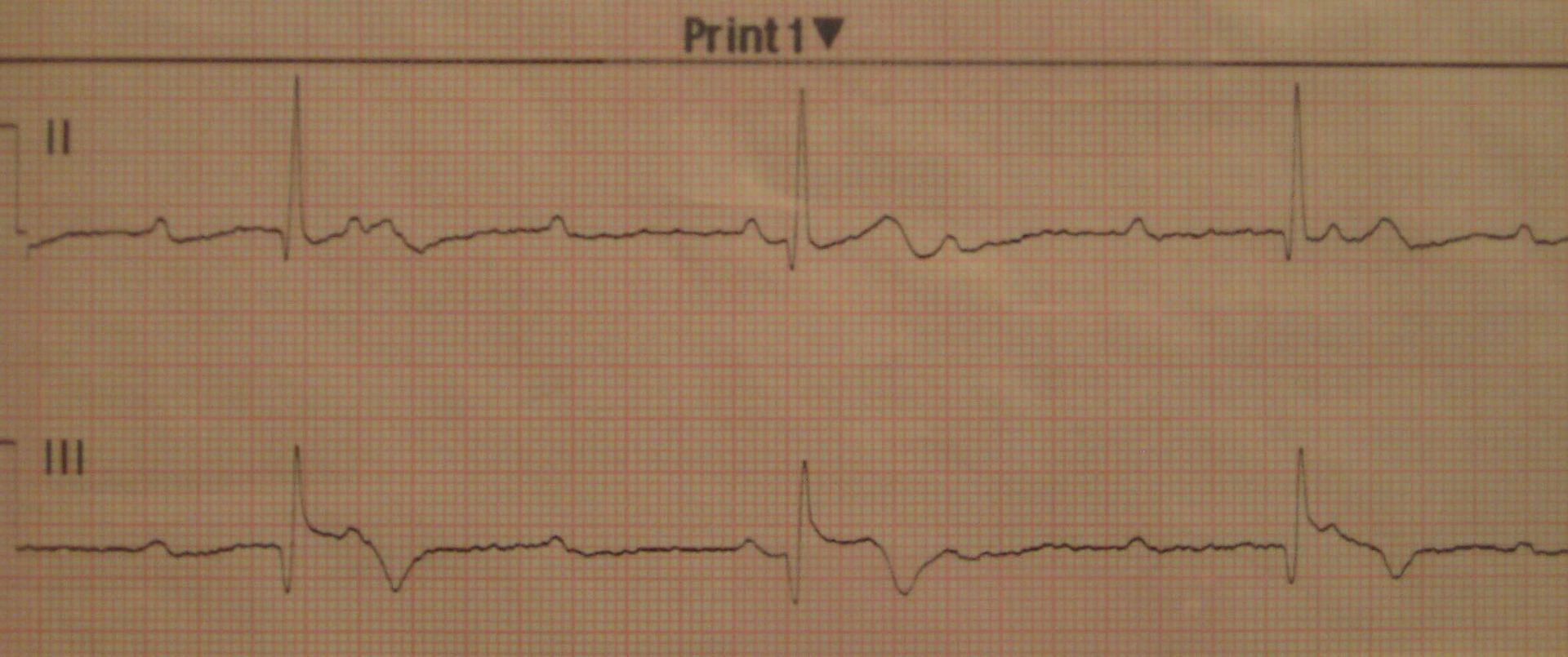
Post resus 3 lead. Second degree heart block type 2...maybe.
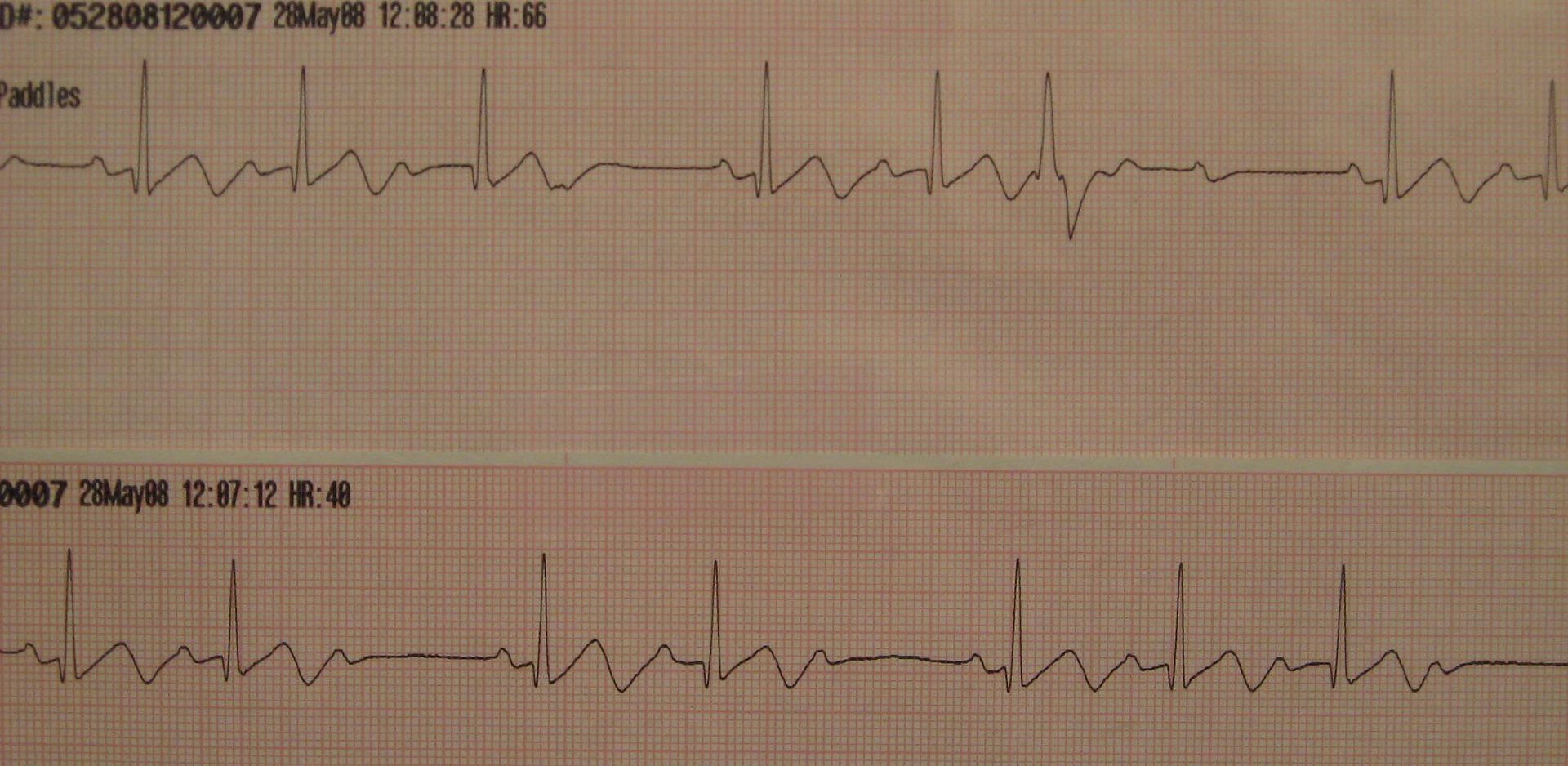
Post resus 12 lead. Now with more elevation and reciprocal depression in leads I and aVL. (may have to click the picture for a clearer view)The helicopter picked him up shortly after, and as he was lead away, I wished him good luck and he thanked me. Amazing. I don't honestly know what happened then. I asked the doctor the next morning what he had heard. He was sorry, but no updates. "That's okay. If I don't know, I'll just write my own ending. It's usually better that way anyway."

Comments
Rock!...
15 lead saves the day again!!!
OMG thank the god(s) for Bob Page!!!
You get 'em!!
Think of how bad it could have been if you were a "cookbook medic" following protocol!
--maaddog
Great post, just one question!
What's a 15 Lead? Where do you place the additional leads?
We do 12 Lead ECG's but I have never heard of a 15 Lead.
Steven